

Goal
The aim of the screening tests is to measure and evaluate cognitive deficits in older subjects and geriatric patients.
It is determined whether the subject’s performance is age-appropriate or whether there are any abnormalities.
In the event of any abnormalities, a specialist (usually a neurologist or neuropsychologist) should always be contacted.
The screening tests were developed by the Cologne University Hospital.

The tests were standardized as part of Yalda Khani’s doctoral dissertation entitled “TabScreen – A Tablet-Based Screening Tool for the Assessment of Cognitive Impairments”, which was completed in 2019 at the Faculty of Medicine of the University of Cologne. The initial normative sample comprised 100 participants, including 52 cognitively unimpaired individuals and 48 individuals with cognitive impairments.
The sample was later expanded to 3,353 participants aged 6 to over 70 years, including 1,551 men and 1,802 women. Children and adolescents aged 6–20 years are very well represented with 1,441 participants, while adults are also strongly represented across all age groups, in particular those aged 20–30 years (591), 40–50 years (407), 50–60 years (367), and 60–70+ years (224). This provides robust normative data for all age groups, enabling precise cognitive assessment across the entire lifespan. (as of August 2025)
Execution
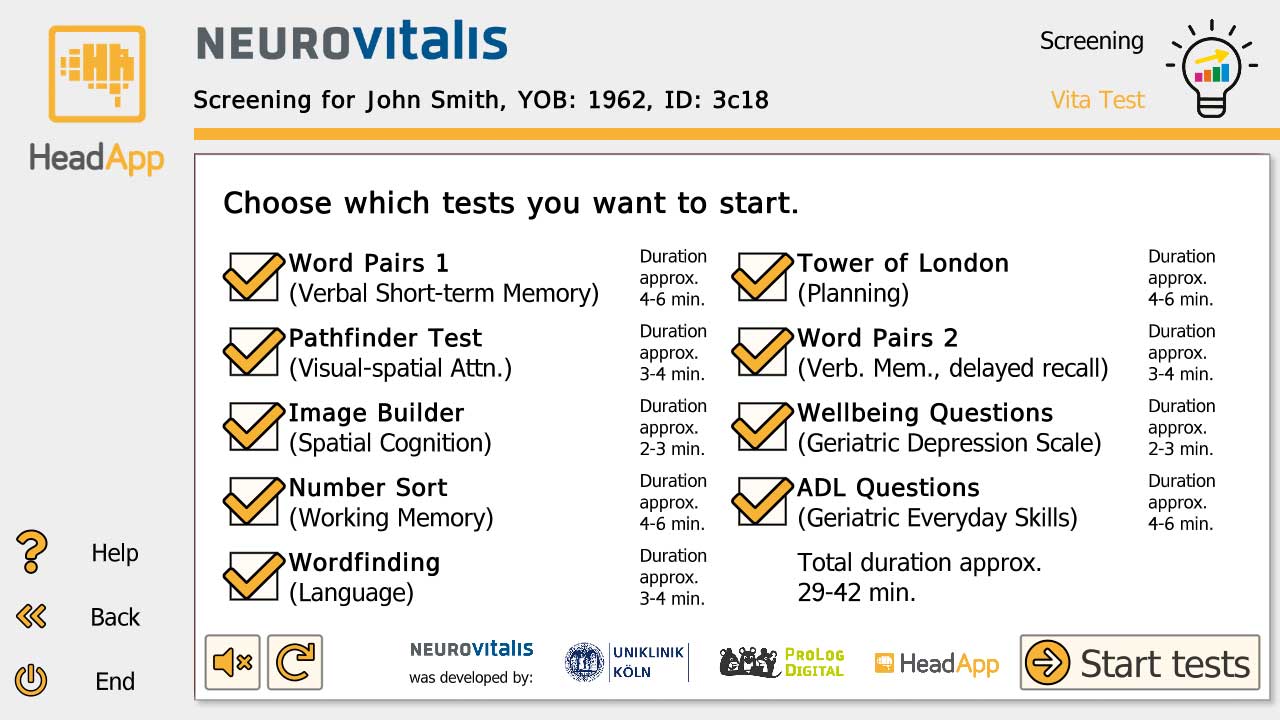
The image (click to enlarge) shows the start of the screening tests. You can choose which individual tests should be carried out.
If all tests are selected, it takes about 30 minutes for healthy volunteers and about 45 minutes (or more) for those affected.
The results are saved and can be viewed later.
There are 3 parallel variants for each test. Nevertheless, each test cannot be repeated for a month after the test to prevent learning effects.
Results
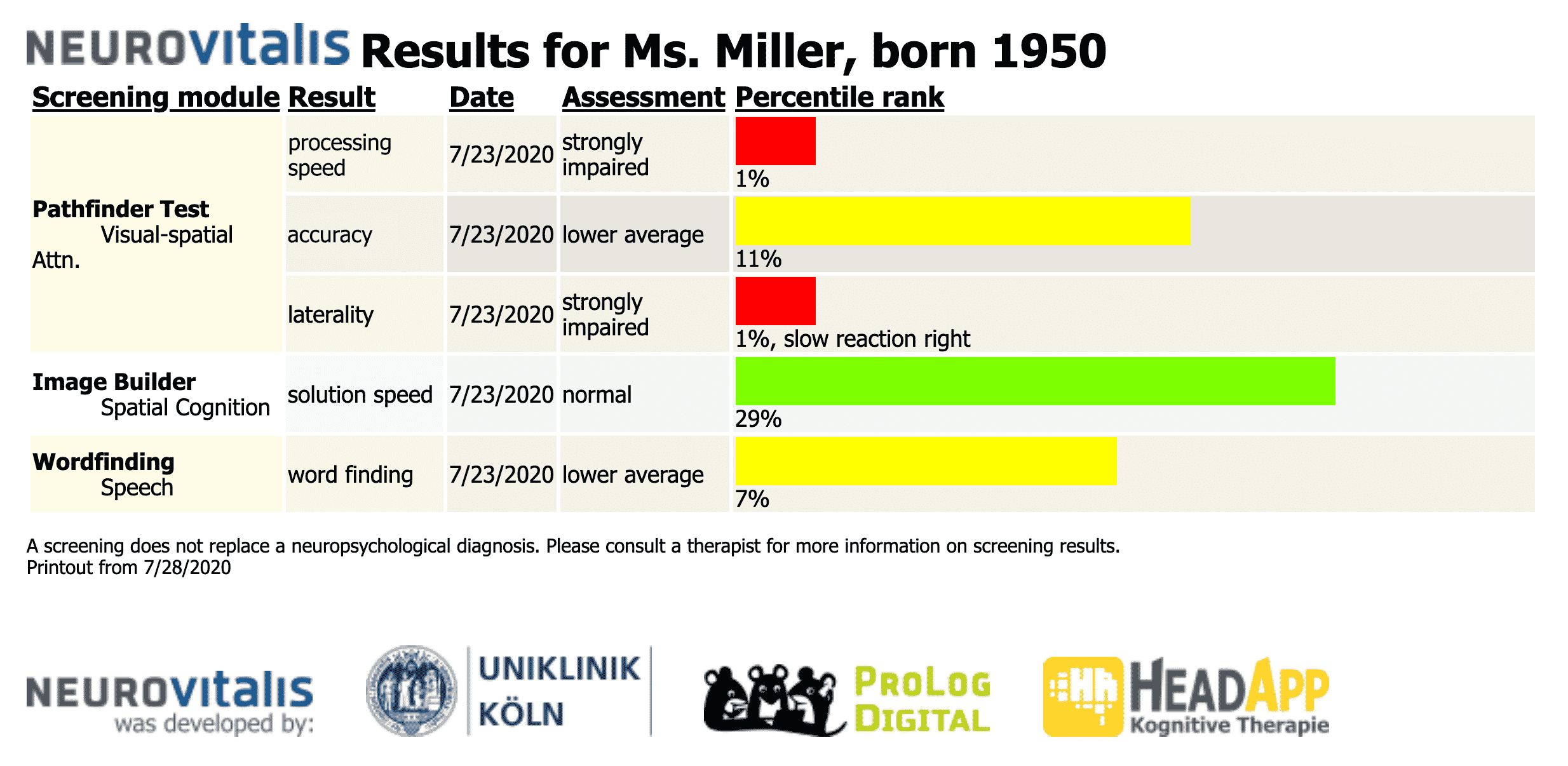
The screening tests are evaluated in a table. The test result of the individual subtests is given as a percentile rank.
If the screening is repeated, the results of the different test times (with a date) appear one below the other. In this way, changes in performance are directly apparent.
Percentile rank
Percentile ranks are commonly used to clarify the interpretation of scores on standardized tests. For the test theory, the percentile rank of a raw score is interpreted as the percentages of examinees in the norm group who scored below the score of interest (Crocker & Algina, 1986).
The HeadApp program interprets the results
with a percentile rank <= 2% as “strongly impaired”
with a percentile rank <= 7% as “impaired”
with a percentile rank <= 16% as “lower average”
all other results as “normal” or better
The colored bars that show the patient’s performance are scaled logarithmically. This ensures that performance improvements in the lower percentile range are more pronounced.
Evaluation of results
The results of the screening are evaluated by HeadApp. If the performance in a test is “lower average” or worse, suitable therapy modules are suggested. When the patient starts training, a level of difficulty is automatically selected that corresponds to the level of performance. If the training offers special setting options, these are carried out according to the test results.
Peculiarity of the test result “laterality”
If the pathfinder test detects a slowdown on the right or left, this indicates a neglect or a hemianopsia.
The basic setting of the patient is changed in accordance with the test results, as a result of which this information affects all therapy programs. If the result is “strongly impaired”, the optokinetic stimulation (OKS) is activated. If the patient cannot tolerate OKS, this must be deactivated manually in the “Patient-> Edit” window.